A herniated disc C4-C5 is less common than bulging and ruptured intervertebral discs at the lower cervical levels of C5/C6 and C6/C7. However, this abnormal disc condition is still quite common and is often found in patients with a noticeable loss of lordotic curvature, since this puts the usually safely situated C4/C5 directly in the ideal location to absorb inordinate amounts of spinal shock.
This dialog will detail herniations and disc degeneration at the middle cervical level of C4/C5. We will explore why intervertebral herniation is commonplace at this specific region of the upper spinal column.
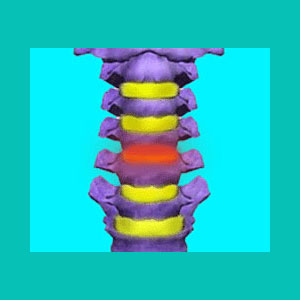
What is a Herniated Disc C4-C5?
C4/C5 is an intervertebral level directly in the middle of the cervical spinal curve. This lordotic curve is designed to protect the body from shock and cushion the spinal structures. When patients lose the spinal curvature, often diagnosed as a loss of lordosis or a hypolordotic curvature, the C4/C5 bears the brunt of much of the cervical movement and must work extra hard to carry and support the substantial weight of the head.
This hypolordosis escalates the normal degenerative processes which act on the cervical spine, causing advanced degenerative disc disease and possibly contributing to herniations at this spinal level. Of course, it is also possible to damage the C4/C5 level even when the cervical lordosis is typical, although this is less common.
Herniated Disc C4-C5 Clinical Profile
Even though C4/C5 bulges are most commonly associated with lordotic changes, they can occur in anyone, due to normal spinal aging or traumatic disc injury. Most C4/C5 herniations are not problematic or painful, like most other locations for herniated discs.
In some cases, a C4/C5 herniations can enact pain through foraminal stenosis of the C5 nerve root, although this condition is far more rare than it is diagnosed. Most commonly, when foraminal stenosis is diagnosed, the disc may block some of the neuroforaminal space, but does not compress the nerve root in any way. In some patients, definitive nerve root compression may occur and can be proven through diagnostic imaging and nerve conduction testing.
Also, the C4/C5 disc can herniate directly into the spinal cord, causing a spinal stenosis condition, although this process is normal to experience in asymptomatic degrees as we get older. When spinal stenosis is diagnosed, the herniated disc may impact the thecal sac, but has no noticeable effect on the actual spinal cord, even if it displaces its normal position. In other cases, true cord compression may result and might produce a diversity of very terrifying symptoms throughout the body.
Bulging Disc C4-C5 Synopsis
True problematic disc prolapse issues at C4/C5 are rare, but many innocent disc bulges do act as scapegoats for many back pain, neck pain, shoulder pain and arm pain syndromes, which are incorrectly diagnosed. In these cases, the herniated disc is surely present, but is coincidental and innocent of sourcing any pain. It is just there.
If your herniated disc treatments for C4/C5 have all failed, I strongly advise you to reconsider your diagnostic conclusion. In these cases, the misdiagnosed herniated disc has you on a fool’s errand seeking relief from a tormentor which is not even the real underlying source of misery. Seek evaluation with a spinal neurologist to prevent this fate from befalling you.
Herniated Disc > Herniated Disc Injury > Herniated Disc C4-C5


